

Building a mental health crisis system in Chicago

What do we mean when we talk about the mental health crisis system?
The mental health crisis system, also called the crisis continuum, is a coordinated system of care designed to provide immediate support, stabilization, and follow-up for people experiencing behavioral health crises, rather than relying on emergency rooms or the criminal legal system.
In Illinois and across the country, this system is built around three core components:
Someone to contact
Services like 988 and other crisis lines provide immediate, accessible support for people in distress.
Someone to respond
Mobile crisis teams and other trained responders provide in-person support to de-escalate situations and connect people to care.
Somewhere to go
Crisis stabilization centers, living rooms, and other safe spaces offer immediate care and support outside of hospitals or jails.
Today, Chicago still does not yet have a scaled, citywide behavioral health response system that can consistently serve as an alternative to law enforcement.
NAMI Chicago has a unique perspective on this work, with a close understanding of how the mental health crisis system operates today and what it will take to improve it.
For more than 20 years, we have worked in partnership with Chicago’s first responder agencies to provide crisis de-escalation training and support policy reform.
We also support Chicagoans in crisis every day through our free Helpline and 988. As a 988 provider, we respond to a large share of calls in Chicago and see firsthand both the strengths of the system and the barriers people face in accessing appropriate care.
The mental health crisis system in Chicago
Each year, thousands of people in Chicago experience a mental health or behavioral health crisis. Each year, thousands of people in Chicago experience a mental health or behavioral health crisis. Despite this level of need, the system remains fragmented, and too many people continue to fall through the cracks. Despite this level of need, the system remains fragmented, and too many people continue to fall through the cracks.
A system still in transition
On August 25, 2021, Illinois Governor J.B. Pritzker signed into law the Community Emergency Services and Supports Act (CESSA), also known as the Stephon Watts Act. CESSA is intended to transform how behavioral health crises are handled, creating a system that provides help, not handcuffs. The current deadline for full implementation is July 1, 2027, but we still have a long way to go to build a fully functioning crisis continuum across Chicago.
Someone to contact
Following years of advocacy, in 2022 the National Suicide Prevention Lifeline became 988. The goal is to provide a simple, easy-to-remember number for behavioral health crises, separate from 911, and to offer a different kind of response for people in need.
988 and 911: What’s the difference?
911 connects callers to emergency dispatchers who assess the situation and send police, fire, or ambulance. It is designed for immediate emergencies where there is a threat to safety.
The launch of 988 in Illinois
The 988 Suicide & Crisis Lifeline launched in Illinois on July 16, 2022. Operated by the Illinois Department of Human Services (IDHS), it provides a 24/7, three-digit dialing code for mental health, substance use, and suicide crises.
In 2023, NAMI Chicago was awarded a grant to become a 988 Crisis Lifeline provider. We began answering calls in January 2024 and now provide 24/7 support, and since have responded to more than 53,000 calls.
This builds on our existing Helpline, which has long supported people in navigating the mental health system. Together, these services allow us to support Cook County residents around the clock. Through this work, we see firsthand how critical it is to have someone to contact and how much more is needed to ensure people can access the right care after that first point of contact.
Someone to respond
The launch of 988 marked an important step toward a more responsive and compassionate crisis system. But it is only one part of a larger continuum. For 988 to be effective, it must be supported by a broader system of care, including mobile crisis teams, stabilization services, and ongoing support. Without these connections, people still struggle to access the care they need after the initial call.
A system still centered on law enforcement
Today, Chicago’s mental health crisis response system is still largely operated by first responders and public safety agencies. Key agencies include:
While these agencies play an important role, the system remains heavily reliant on law enforcement. Across the country, including in Chicago, police already spend a significant portion of their time responding to behavioral health-related calls. These interactions are often not designed to provide care and can increase the risk of harm for people experiencing mental health crises.
There is growing consensus that communities need a fourth option: a behavioral health response that can operate alongside other first responders to reduce the risk of harm to all involved, and divert people experiencing crisis away from the legal system and toward the help they need to recover.
The CARE model: A step toward co-response
Chicago began moving in this direction with the launch of the Crisis Assistance Response and Engagement (CARE) pilot in 2021. CARE introduced a co-response model that brought together community paramedics, mental health clinicians, and Crisis Intervention Team (CIT) trained police officers. These multidisciplinary teams responded to 911 calls with a mental health component, aiming to provide a more appropriate, health-focused response.
The pilot also included alternate response teams and follow-up services, showing early progress in building coordination across agencies and creating a different kind of response in the community. While limited in geography and hours, CARE represented an important step toward reducing reliance on law enforcement and improving how Chicago responds to crises.
That early progress has not been sustained. In September 2024, the City removed police officers from CARE teams in an effort to reduce law enforcement involvement in behavioral health emergencies. While well-intentioned, this change has not produced a fully functional alternative response system. As a result:
Other behavioral health response options
Somewhere to go
Even when someone is able to reach support and receive an in-person response, the system still depends on having safe, appropriate places where people can go for care. Too often, the default options are emergency rooms or no placement at all.
Limited options for care and stabilization
Emergency rooms are not designed to provide ongoing behavioral health care, and they are often the only option available during a crisis. Without a broader network of community-based settings, people experience long wait times, repeated crises, or are discharged without the support they need to stay well. A strong crisis system requires accessible, community-based options that focus on stabilization and recovery, not just immediate safety.
Types of crisis care settings
Strengthening access to follow-up care
Expanding crisis care settings is only part of the solution. Even when people are able to access care during a crisis, they often face delays, administrative barriers, and gaps in follow-up support once they leave that initial setting.
HB4495 is designed to address this gap by allowing immediate access to certain mental health services following a behavioral health crisis. The bill enables a crisis assessment to provide up to 30 days of care without requiring a full, lengthier assessment process. This includes services such as:
This approach helps people stay connected to care during a critical period after a crisis by reducing delays and administrative barriers.
How we build a better system
There is no single solution to improving Chicago’s mental health crisis system. Building a strong, coordinated continuum of care will require sustained investment, cross-sector coordination, and a clear focus on connecting people to care beyond the moment of crisis.
Chicago has made progress, but key gaps remain across all parts of the system.
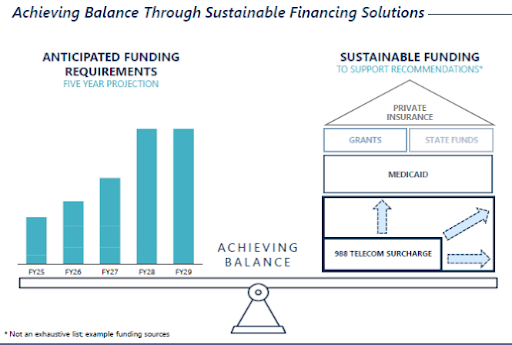
Funding the new system
YOU MIGHT BE INTERESTED IN
988 and crisis support
Get immediate support for mental health or emotional distress. Learn how 988 works and how to access help for yourself or someone you care about.
Policy & advocacy
We’re working to strengthen the crisis continuum across Illinois by advocating for sustained investment in 988, mobile crisis response, and community-based care.
Recovery & wellness
Many people reach crisis because of gaps in housing, health care, and community support. We’re working to strengthen the mental health system and reduce reliance on crisis care.